Retinoids, Tretinoin and retinol – everything you need to know

Overview
Thanks to their ability to maintain healthy, glowing skin, retinoids are widely prescribed by dermatologists for a variety of skin conditions and are found, in abundance, in all kinds of cosmetics. Here we give you an up to date review on everything you need to know about retinoids and how to use them.
What are retinoids?
Retinoids are a large family of synthetic and naturally occurring compounds derived from vitamin A. Retinol, Tretinoin (as well as others such as retinaldehyde) are all types of retinoid. Their ability to regulate a number of key processes in the skin was discovered as far back as World War 1. Since then they have been used in the treatment of skin conditions such as acne and more recently (over the last two decades), to support the skin’s ageing process. Their function in the skin is vast and they are able to:
- Treat acne spots such as comedones, papules and pustules by increasing skin cell turnover as well as helping to break down dead skin cells and debris blocking the hair follicles. They also help to regulate the amount of oil produced by the skin’s oil glands as well as the amount of keratin (a sticky protective protein) produced by the skin.
- Improve the appearance of fine lines and wrinkles by stimulating the production of collagen.
- Improving skin glow through their exfoliant properties and helping discolouration and inflammation of the skin.
- Improve skin firmness through their ability to stimulate collagen and influence epithelial cell growth.
- Help fight hyperpigmentation by blocking the production of the pigment melanin as well as reducing the amount of excess melanin in the skin through its action of boosting skin cell turnover.
- Reduce the appearance of pores by increasing skin cell turnover, boosting collagen and helping break down dead skin cells and oil that build up in pores.
Are all retinoids the same?
Not all retinoids are equal and they differ in their structure, their strength and therefore in effectiveness.
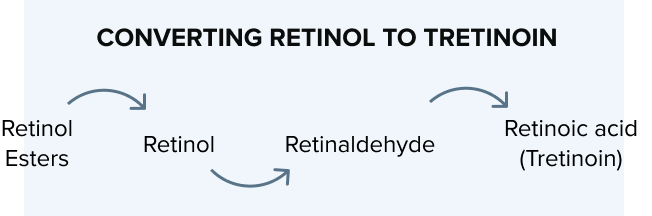
All retinoids need to be converted (by skin enzymes) to retinoic acid (Tretinoin) which then exerts its effects by activating retinoic acid and retinoid X receptors found on skin cells. The conversion of retinol to retinoic acid is slow and varies between individuals. This is the reason why most over the counter retinoids will be less effective than their prescription strength counterparts and why it takes longer to see results.
Tretinoin is the most powerful retinoid available as it doesn’t require conversion to retinoic acid – because it already is retinoic acid. Tretinoin has been used in clinical practice for the longest amount of time so has decades of evidence supporting its efficacy. Other powerful retinoids include Adapalene which is mainly used in the treatment of acne and is available on prescription in the UK. Retinol (and its derivatives retinyl and retinal) are amongst the most commonly used ingredients in skin-ageing cosmetics and are available over the counter. They have been shown to be 20 times less potent than Tretinoin.
Types of Retinoids
Retinol esters
(Retinyl Palmitate, Retinyl Propionate, Retinyl-Retinoate)
Gentle retinoids suitable for even the under eye area. There’s little evidence for their effectiveness.
Available over the counter.
Retinol
Has efficacy for ageing concerns when used long term, can be irritant depending on preparation, very unstable when exposed to light oxygen or heat so difficult to formulate well.
Available over the counter.
Retinaldehyde
(Retinylaldehyde)
Generally well tolerated but with weak efficacy for ageing concerns.
Available over the counter.
Retinoic acid
(Tretinoin)
Tretinoin is used for acne and ageing concerns and is the most studied retinoid and regarded as the most effective but can be more irritant than Adapalene.
Available on prescription.
Adapalene
(Differin)
Adapalene has been approved for the treatment of acne but there is less evidence for its effect on ageing.
Available on prescription.
Retinoic acid esters
(Granactive Retinoid, Hydroxypinacolone Retinoate)
Currently little evidence as new and no sufficient studies available.
Available over the counter.
Another factor that can influence the effectiveness of a retinoid is the formulation. Retinoids can be found in creams, gels and serums with creams being generally the more hydrating preparation and less irritant. Gel formulations allow for quicker penetration of the retinoid which also increases effectiveness. They can be drying and are generally the preferred vehicle for oily skin types.
Retinoids and Acne
Retinoids (such as Tretinoin and Adapalene ) are an effective and crucial treatment in acne as they inhibit the formation of microcomedones-small invisible bumps that are thought to be the primary lesion of acne (1). Retinoids also have anti-inflammatory properties and are effective against the inflammatory lesions in acne such as the red spots and painful nodules (2).
Adapalene and Tretinoin are the two most commonly used retinoids that are available in the UK on prescription only and they come in a variety of formulations (such as creams, gels) and also concentrations. The type of topical retinoid prescribed by your healthcare professional will depend on a number of factors such as severity of acne, previous use of retinoids, how well it is tolerated and your skin type. Multiple clinical trials have shown the efficacy of topical retinoids in the treatment of acne (3, 4, 5, 6, 7).
Combination therapy is preferred in the treatment of acne
Several studies have shown that treatment with a combination of topical retinoids and antimicrobials such as clindamycin or benzoyl peroxide has improved treatment benefit (8, 9).
Retinoids and ageing
Topical retinoids are the gold standard with the most evidence based treatment success for the treatment of the visible signs of ageing. Tretinoin is by far the most extensively studied retinoid and concentration from 0.01 to 0.1% have been studied with good effect (10, 11, 12, 13, 14). Tretinoin needs to be applied regularly and for a minimum of 16 weeks before assessing the effects. Studies evaluating its safety in 204 subjects over a two year period found no evidence for concern with long term use (13).
How to use a retinoid
Retinoids are applied once daily and should be applied at night as they can be unstable in sunlight. This is particularly true for Tretinoin whilst Adapalene is more stable in light.
Skin irritation is a common expected side effect of retinoids particularly during the first month of use (15). To minimise the side effects we advise you start with the lowest concentration of Tretinoin recommended for your skin which will be determined by your prescriber based on a number of factors including skin type, previous retinoid use, skin concern and any other skin conditions that may affect treatment. The potency of the retinoid will typically increase gradually and as tolerated. If you have a history of sensitive skin you may benefit from lower initial concentrations.
Retinoids should be applied as a thin layer on cleansed skin after it has been thoroughly dried (16). Our Daily Doser has been cleverly designed to dispense the exact amount you need each night to cover the entire face.
When starting off your retinoid journey we advise to avoid any other active skincare ingredients in particular exfoliants such as AHA/BHAs and harsh cleansers or toners to minimise the risk of irritation (17). These products can later be introduced once retinoids are tolerated to maximise the benefit of both active ingredients.
We advise that you use a non-comedogenic moisturiser 10 minutes after the application of your retinoid to further minimise the effects of irritation which is particularly important during the first month of use but also during the winter months when retinoids can be less tolerated and irritation is more common.
Prescription retinoids and over the counter retinoids can’t be used in pregnancy or when breastfeeding and need to be avoided due to the risk of congenital abnormalities in infants with its use.
References
- Management of acne: a report from a Global Alliance to Improve Outcomes in Acne.
Gollnick H, Cunliffe W, Berson D, Dreno B, Finlay A, Leyden JJ, Shalita AR, Thiboutot D, Global Alliance to Improve Outcomes in Acne , J Am Acad Dermatol. 2003;49(1 Suppl):S1. - Topical retinoids in inflammatory acne: a retrospective, investigator-blinded, vehicle-controlled, photographic assessment. Leyden JJ, Shalita A, Thiboutot D, Washenik K, Webster G. Clin Ther. 2005;27(2):216.
- Comparison of two concentrations of Tretinoin solution in the topical treatment of acne vulgaris.
Krishnan G , Practitioner. 1976;216(1291):106. - A combined analysis of 2 randomized clinical studies of Tretinoin gel 0.05% for the treatment of acne.
Webster G, Cargill DI, Quiring J, Vogelson CT, Slade HB
Cutis. 2009;83(3):146. - Adapalene gel 0.3% for the treatment of acne vulgaris: a multicenter, randomized, double-blind, controlled, phase III trial.
Thiboutot D, Pariser DM, Egan N, Flores J, Herndon JH Jr, Kanof NB, Kempers SE, Maddin S, Poulin YP, Wilson DC, Hwa J, Liu Y, Graeber M, Adapalene Study Group. J Am Acad Dermatol. 2006;54(2):242. - Efficacy and tolerance of Adapalene cream 0.1% compared with its cream vehicle for the treatment of acne vulgaris. Lucky A, Jorizzo JL, Rodriguez D, Jones TM, Stewart DM, Tschen EH, Kanof NB, Miller BH, Wilson DC, Loven KH Cutis. 2001;68(4 Suppl):34.
- Adapalene 0.1% lotion in the treatment of acne vulgaris: results from two placebo-controlled, multicenter, randomized double-blind, clinical studies.Eichenfield LF, Jarratt M, Schlessinger J, Kempers S, Manna V, Hwa J, Liu Y, Graeber M, Adapalene Lotion Study Group
J Drugs Dermatol. 2010;9(6):639. - Two randomized, double-blind, controlled trials of 2219 subjects to compare the combination clindamycin/Tretinoin hydrogel with each agent alone and vehicle for the treatment of acne vulgaris. Leyden JJ, Krochmal L, Yaroshinsky A J Am Acad Dermatol. 2006;54(1):73. Epub 2005 Nov 28.
- Efficacy and tolerability of combined topical treatment of acne vulgaris with Adapalene and clindamycin: a multicenter, randomized, investigator-blinded study.Wolf JE Jr, Kaplan D, Kraus SJ, Loven KH, Rist T, Swinyer LJ, Baker MD, Liu YS, Czernielewski J J Am Acad Dermatol. 2003;49(3 Suppl):S211.
- Photoaging.
Han A, Chien AL, Kang S
Dermatol Clin. 2014;32(3):291. - Interventions for photodamaged skin.
Samuel M, Brooke RC, Hollis S, Griffiths CE
Cochrane Database Syst Rev. 2005; - Long-term treatment of photoaged human skin with topical retinoic acid improves epidermal cell atypia and thickens the collagen band in papillary dermis.
Cho S, Lowe L, Hamilton TA, Fisher GJ, Voorhees JJ, Kang S
J Am Acad Dermatol. 2005;53(5):769. - Long-term efficacy and safety of Tretinoin emollient cream 0.05% in the treatment of photodamaged facial skin: a two-year, randomized, placebo-controlled trial. .Kang S, Bergfeld W, Gottlieb AB, Hickman J, Humeniuk J, Kempers S, Lebwohl M, Lowe N, McMichael A, Milbauer J, Phillips T, Powers J, Rodriguez D, Savin R, Shavin J, Sherer D, Silvis N, Weinstein R, Weiss J, Hammerberg C, Fisher GJ, Nighland M, Grossman R, Nyirady J
Am J Clin Dermatol. 2005;6(4):245-53. - Two concentrations of topical Tretinoin (retinoic acid) cause similar improvement of photoaging but different degrees of irritation. A double-blind, vehicle-controlled comparison of 0.1% and 0.025% Tretinoin creams.
Griffiths CE, Kang S, Ellis CN, Kim KJ, Finkel LJ, Ortiz-Ferrer LC, White GM, Hamilton TA, Voorhees JJ
Arch Dermatol. 1995;131(9):1037. - Kang S, Voorhees JJ. Topical retinoids. In: Fitzpatrick’s Dermatology in General Medicine, 7th ed, Wolff K, Goldsmith LA, Katz SI, et al (Eds), McGraw Hill, 2008. P.2106.
- Mukherjee S, Date A, Patravale V, Korting HC, Roeder A, Weindl G. Retinoids in the treatment of skin aging: an overview of clinical efficacy and safety. Clinical interventions in aging. 2006 Dec;1(4):327.
- Hetland RB, Granum B, Lutzow-Holm C, Lyche JL, Paulsen JE, Thrane V, Alexander J, Binderup ML, Dahl KH, Husøy T, Sanner T. Risk assessment of vitamin A (retinol and retinyl esters) in cosmetics. Opinion of the Panel on Food Additives, Flavourings, Processing Aids, Materials in Contact with Food and Cosmetics of the Norwegian Scientific Committee for Food Safety. VKM Report. 2012.